Bringing Whole Genome and Transcriptome Sequencing into Diagnostic Workup for Sarcoma and Paediatric Cancer Patients
By Svetlana Nikic
In the evolving field of precision oncology, Whole Genome and Transcriptome Sequencing (WGTS) is stepping out of research labs and into clinical practice. Traditionally considered complex and resource-intensive, WGTS is increasingly recognized for its ability to provide a comprehensive molecular profile as a single test, particularly valuable in cancers where actionable targets are rare or difficult to identify through standard methods.
In this short blog, I am exploring why sarcoma and paediatric cancer patients may benefit most from the clinical integration of WGTS, and how this shift could transform diagnostic pathways, therapeutic decisions, and long-term patient outcomes. Additionally, I am highlighting data from recently presented poster at AACR 2025 “Whole genome and transcriptome sequencing can be introduced into the diagnostic workup of sarcoma and paediatric cancer patients”, developed jointly with Kristine Jinnett, PhD from Kristine Jinnett Consulting, where we carried out a meta-analysis of all published scientific work so far, which highlighted the diagnostic and clinical added value of WGTS in comparison to traditional methods, in sarcoma and paediatric cancer patients1-12.
Why Focus on Sarcomas and Paediatric Cancers?
Diagnosing sarcomas using traditional methods is challenging since this cancer type is highly heterogenous1,2 and often requires more than just morphological evaluation and immunohistochemistry (IHC). Paediatric cancers, while rare, represent the second leading cause of death in children, and those with longer survival frequently suffer from long-term, treatment induced side effects, impacting significantly their quality of life13.
Both sarcomas and paediatric cancers are characterized by low mutation burdens, a high prevalence of structural variations (SVs), and unusual molecular drivers 14. These features make them uniquely challenging to diagnose using conventional methods such as FISH, IHC, single-gene tests and targeted NGS panels. The suboptimal molecular profiling can lead to misdiagnosis and delay in treatment initiation.
For these patients, WGTS which integrates whole-genome sequencing (WGS) and whole transcriptome sequencing (WTS) into a single workflow, offers a panoramic view of the alterations at DNA and RNA level by capturing gene fusions, copy number alterations (CNAs), enhancer hijacking, SVs, differential gene expression and large genomic signatures such as HRD as well as emerging ones, that can be informative of changes in tumour micro-environment and can provide insights into tumour biology relevant for patient classification, diagnosis and potentially long-term outcomes.
How WGTS Enhances Clinical Decision-Making
Based on our meta-analysis of published studies which focused on demonstrating the clinical impact of WGTS in comparison to Standard of care (SoC), we have identified several clinical scenarios where this integrated approach adds clear value:
- Change or Refinement of initial diagnosis: Refinement / change of diagnosis when compared to SoC ranged from 3%-37% (av 18.6%) and 5.2%-51% of patients (av 20.6%) in sarcoma and paediatric cancer patients, respectively.
- Therapeutic stratification: WGTS provides additional insights into therapy-informing findings in 4-67% of patients, when compared to SoC.
- Germline findings: WGTS workflow includes sequencing of both normal and tumour DNA, enabling identification if inherited variants which are important for patient and its family management. In our meta-analysis we found that on average, the analysed studies reported germline findings in 7.35% of patients.
From Pilot Programs to Implementation
While WGTS is not yet standard molecular testing approach across oncology care, several countries, including the Netherlands, UK, Sweden and Australia, have launched pilot programs that integrate WGTS into clinical diagnostics for rare and complex cancers, including sarcomas and paediatric cancer patients. These initiatives demonstrate that, with appropriate infrastructure WGTS can be performed within clinically acceptable turnaround times (10–14 days) and at competitive costs relative to the value it provides. Currently, the Netherlands is the only country where WGS is reimbursed for all patients with cancers of unknown primary (CUP). However, uptake remains slow, largely due to limited awareness and understanding of the diagnostic and clinical value that this approach can offer to both the healthcare system and, most importantly, to patients.
Integrating WGTS into routine diagnostics is not without challenges. These include:
- Regulatory hurdles and reimbursement: Current HTA models are slow to adapt to multiomic approaches.
- Data interpretation and reporting standards: Harmonization is needed to ensure consistent clinical actionability with regards to tiering of clinically actionable alterations.
- Workflow harmonization: There’s a need for developing a clinical grade and NGS-agnostic WGTS workflow with well defined quality control metric to ensure reproducibility and consistency.
- Clinical workforce education: Oncologists and pathologists need support to interpret and apply WGTS findings effectively.
Despite current hurdles, the momentum behind WGTS is undeniable. With the right infrastructure, stakeholder alignment, and implementation strategy, WGTS has the potential to evolve from a “nice-to-have” into a standard-of-care tool for select cancer types. More than just a technological advancement, WGTS marks a shift toward diagnostic completeness and efficiency, delivering more accurate diagnoses and therapy-informing insights that ultimately improve patient outcomes.
- Prendergast SC, Strobl AC, Cross W, et al. Sarcoma and the 100,000 Genomes Project: our experience and changes to practice. J Pathol Clin Res. Oct 2020;6(4):297-307. doi:10.1002/cjp2.174
- Schipper LJ, Monkhorst K, Samsom KG, et al. Clinical Impact of Prospective Whole Genome Sequencing in Sarcoma Patients. Cancers (Basel). Jan 16 2022;14(2)doi:10.3390/cancers14020436
- Watkins JA, Trotman J, Tadross JA, et al. Introduction and impact of routine whole genome sequencing in the diagnosis and management of sarcoma. Br J Cancer. Sep 2024;131(5):860-869. doi:10.1038/s41416-024-02721-8
- Öfverholm I, Wallander K, Haglund C, et al. Comprehensive Genomic Profiling Alters Clinical Diagnoses in a Significant Fraction of Tumors Suspicious of Sarcoma. Clin Cancer Res. Jun 14 2024;30(12):2647-2658. doi:10.1158/1078-0432.Ccr-24-0384
- Andrew EC, Lewin J, Desai J, et al. Clinical Impact of Comprehensive Molecular Profiling in Adolescents and Young Adults with Sarcoma. J Pers Med. Jan 23 2024;14(2)doi:10.3390/jpm14020128
- Wong M, Mayoh C, Lau LMS, et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat Med. Nov 2020;26(11):1742-1753. doi:10.1038/s41591-020-1072-4
- Newman S, Nakitandwe J, Kesserwan CA, et al. Genomes for Kids: The Scope of Pathogenic Mutations in Pediatric Cancer Revealed by Comprehensive DNA and RNA Sequencing. Cancer Discov. Dec 1 2021;11(12):3008-3027. doi:10.1158/2159-8290.Cd-20-1631
- Trotman J, Armstrong R, Firth H, et al. The NHS England 100,000 Genomes Project: feasibility and utility of centralised genome sequencing for children with cancer. Br J Cancer. Jul 2022;127(1):137-144. doi:10.1038/s41416-022-01788-5
- Shukla N, Levine MF, Gundem G, et al. Feasibility of whole genome and transcriptome profiling in pediatric and young adult cancers. Nat Commun. May 18 2022;13(1):2485. doi:10.1038/s41467-022-30233-7
- Villani A, Davidson S, Kanwar N, et al. The clinical utility of integrative genomics in childhood cancer extends beyond targetable mutations. Nat Cancer. Feb 2023;4(2):203-221. doi:10.1038/s43018-022-00474-y
- Wadensten E, Wessman S, Abel F, et al. Diagnostic Yield From a Nationwide Implementation of Precision Medicine for all Children With Cancer. JCO Precis Oncol. Jun 2023;7:e2300039. doi:10.1200/po.23.00039
- Hodder A, Leiter SM, Kennedy J, et al. Benefits for children with suspected cancer from routine whole-genome sequencing. Nature Medicine. 2024;30(7):1905-1912. doi:10.1038/s41591-024-03056-w
- Zahnreich S, Schmidberger H. Childhood Cancer: Occurrence, Treatment and Risk of Second Primary Malignancies. Cancers (Basel). May 26 2021;13(11)doi:10.3390/cancers13112607
- Gröbner SN, Worst BC, Weischenfeldt J, et al. The landscape of genomic alterations across childhood cancers. Nature. Mar 15 2018;555(7696):321-327. doi:10.1038/nature25480
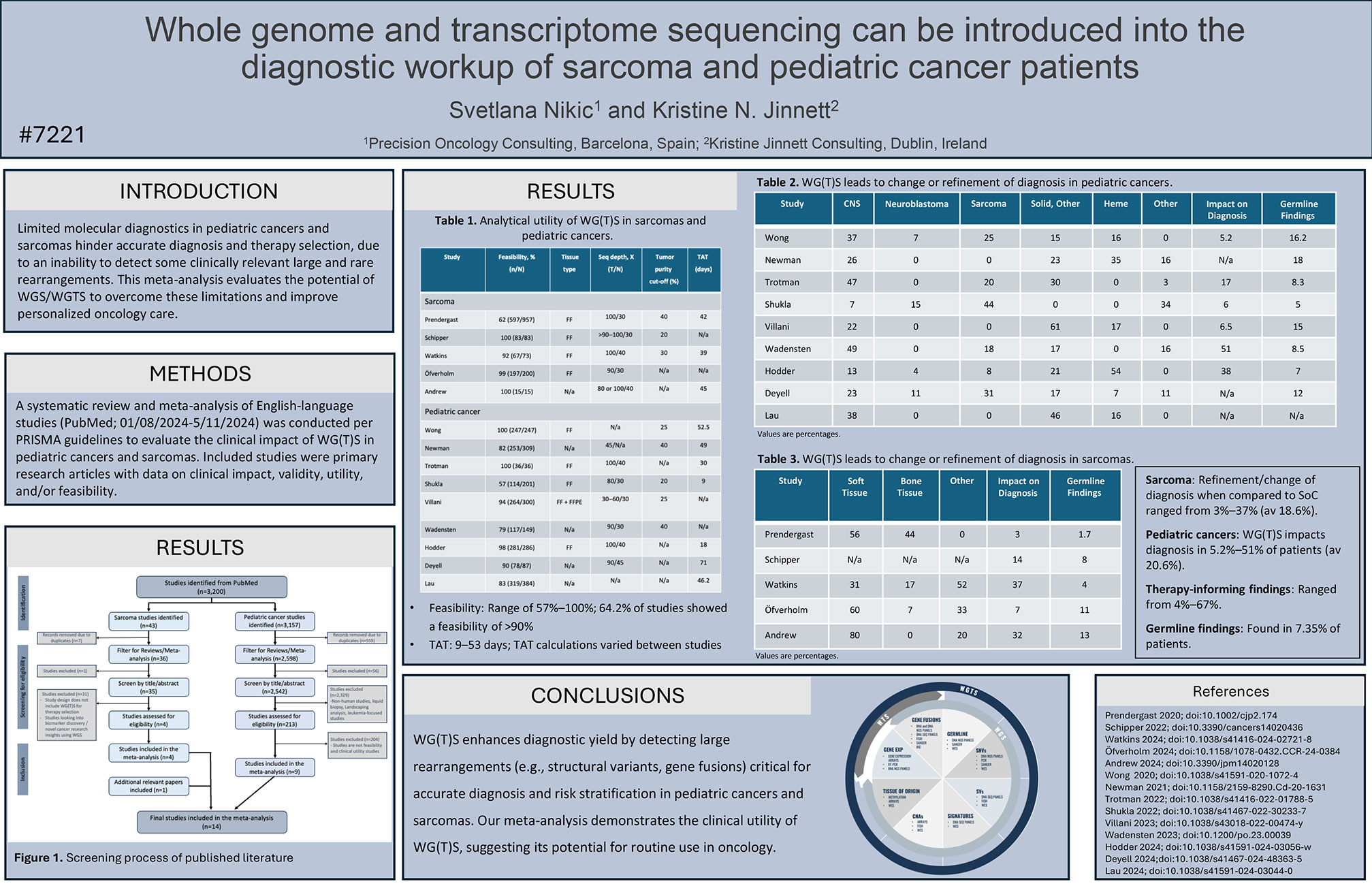
AACR Annual Meeting 2025 – Poster #7221
Whole genome and transcriptome sequencing can be introduced into the diagnostic workup of sarcoma and pediatric cancer patients.